
This is what Michael Caine has to say on the matter:I feel the Dutch are not being mentioned enough you chauvinist pigs!
Coronavirus COVID-19 Thread
- Thread starter Jolly_Green_Giant
- Start date
-
- Tags
- coronavirus virus wuflu

My-Cocaine!
Todays numbers from the UK 21st of May 2020:
Total confirmed 250,908 with 2,615 new, total dead 36,042 with 338 new.
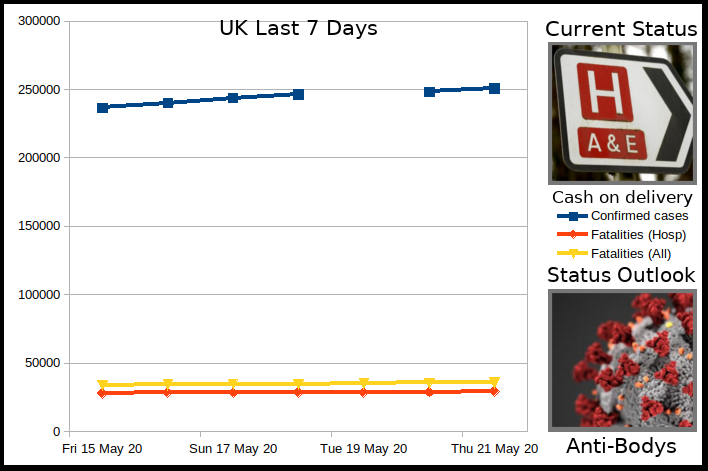
The current status is bought to us by the news the UK government has decided to scrap a surcharge that a significant portion of the Health Service staff were being charged so they could actually use the health service - It transpires any foreign worker coming to work in the UK has to pay a charge up front, £400 a year now raising to over £600 nearer the end of the year to be able to use the NHS. This ignores the fact that as workers in the UK, their taxes go to paying for the NHS anyway. Paying twice? Not the health workers any more, at least:

 www.bbc.co.uk
www.bbc.co.uk
The status outlook is bought to us by a concerning study from our favorite unlockdownable friends the Swedes. Testing performed in April suggests by the end of that month only 7.3% of the residents of Stockholm had antibodies to defend them from COVID-19. They had been expecting closer to 20% by May 1st. If the results are correct and it is the case that such a small number acquire immunity with each wave, even rounding it up to an eventual 10% you are looking at perhaps five or six waves (years, if it's seasonal and strikes hardest in winter) before immune numbers are at the level where Heard Immunity (which they are definitely not trying to achieve) can defend the population, assuming the pathogen does not then mutate into another strain which will start the cycle all over again:

 www.theguardian.com
www.theguardian.com
Does this set the front-loading-deaths theory back a bit...?
Total confirmed 250,908 with 2,615 new, total dead 36,042 with 338 new.
The current status is bought to us by the news the UK government has decided to scrap a surcharge that a significant portion of the Health Service staff were being charged so they could actually use the health service - It transpires any foreign worker coming to work in the UK has to pay a charge up front, £400 a year now raising to over £600 nearer the end of the year to be able to use the NHS. This ignores the fact that as workers in the UK, their taxes go to paying for the NHS anyway. Paying twice? Not the health workers any more, at least:
NHS fees to be scrapped for overseas health staff and care workers
NHS staff and care workers from abroad are to be exempt, as Labour calls it "the right thing to do".
The status outlook is bought to us by a concerning study from our favorite unlockdownable friends the Swedes. Testing performed in April suggests by the end of that month only 7.3% of the residents of Stockholm had antibodies to defend them from COVID-19. They had been expecting closer to 20% by May 1st. If the results are correct and it is the case that such a small number acquire immunity with each wave, even rounding it up to an eventual 10% you are looking at perhaps five or six waves (years, if it's seasonal and strikes hardest in winter) before immune numbers are at the level where Heard Immunity (which they are definitely not trying to achieve) can defend the population, assuming the pathogen does not then mutate into another strain which will start the cycle all over again:
Just 7.3% of Stockholm had Covid-19 antibodies by end of April, study shows
Official findings add to concerns about Sweden’s laissez-faire strategy towards the pandemic
www.theguardian.com
Does this set the front-loading-deaths theory back a bit...?
Last edited:
The article seems relevant, but even the author admits there may be assumption errors. My biggest question, maybe I missed it, is what percentage of the target population was tested and if the tests are accurate. I know I have seen articles where they say the antibody tests are still a little unreliable, with as much as 60% false positives (can't remember where I read it). Another possible reason, is maybe people are not developing antibodies like we expect... we have only been at this for 3 months... this stuff takes time.The status outlook is bough to us by a concerning study from our favorite unlockdownable friends the Swedes.
“It means either the calculations made by the agency and myself are quite wrong, which is possible, but if that’s the case it’s surprising they are so wrong,” he told the newspaper Dagens Nyheter. “Or more people have been infected than developed antibodies.”
Details of the study are hereThe article seems relevant, but even the author admits there may be assumption errors. My biggest question, maybe I missed it, is what percentage of the target population was tested and if the tests are accurate. I know I have seen articles where they say the antibody tests are still a little unreliable, with as much as 60% false positives (can't remember where I read it). Another possible reason, is maybe people are not developing antibodies like we expect... we have only been at this for 3 months... this stuff takes time.
“It means either the calculations made by the agency and myself are quite wrong, which is possible, but if that’s the case it’s surprising they are so wrong,” he told the newspaper Dagens Nyheter. “Or more people have been infected than developed antibodies.”


Första resultaten från pågående undersökning av antikroppar för covid-19-virus — Folkhälsomyndigheten
Det är vanligast att personer mellan 20 och 64 år har genomgått en infektion med covid-19, jämfört med personer i övriga åldersgrupper. Det visar de första resultaten från Folkhälsomyndighetens undersökning av förekomst av antikroppar mot viruset i blodprover.
And with Googles wonderful translation system:
EDIT - well, perhaps Google isn't so wonderful as that link doesn't work. Pop the URL in that translation page somehow

Last edited:
This is all still very much in the air. We're still playing on version 1.0 with antibody tests... there is still a lot of work to be done. Some good articles attached.
Understanding the startling rates of false positives and false negatives for tests that seem, on the surface, to be quite accurate could have profound consequences for health policy as we travel deeper into this pandemic. Failing to do our mathematical due diligence has the potential to take us past the tipping point beyond which the epidemic starts to grow again, leading to even more avoidable deaths.
The first commercial antibody tests to gain the FDA’s nod — from Cellex, Ortho Clinical Diagnostics and Chembio Diagnostic Systems — have sensitivity rates from 94 to 100 percent. The higher the sensitivity, the less likely a test is to give a false negative result — saying someone doesn’t have antibodies when they really do. A person may also get a false negative result if they’re tested too early, before antibodies begin to accumulate around one to two weeks into an infection.
Part of the challenge with specificity in this context is that SARS-CoV-2 is not the only member of the coronavirus family to infect human beings. Two other coronaviruses, SARS and MERS, caused earlier multi-country outbreaks. Moreover, there are at least four coronaviruses that cause a fraction of cases of the common cold.
With SARS-CoV-2 so new, it’s hard to be sure. Not all infections create immunity; tetanus, for example, often doesn’t.
Those data seem to indicate that 4 to 5 percent of people in those places had already been exposed, giving Covid-19 a fatality rate closer to 0.1 to 0.2 percent. But those studies, which have not yet been reviewed by other scientists, have come under fire, partly due to the high rate of mistaken results in the test, which has not undergone FDA review and has a known tendency toward false positives.
This one is a really good read, packed with info

 www.discovermagazine.com
www.discovermagazine.com

 www.the-scientist.com
www.the-scientist.com

 www.scilifelab.se
www.scilifelab.se

 theconversation.com
theconversation.com
Understanding the startling rates of false positives and false negatives for tests that seem, on the surface, to be quite accurate could have profound consequences for health policy as we travel deeper into this pandemic. Failing to do our mathematical due diligence has the potential to take us past the tipping point beyond which the epidemic starts to grow again, leading to even more avoidable deaths.
The first commercial antibody tests to gain the FDA’s nod — from Cellex, Ortho Clinical Diagnostics and Chembio Diagnostic Systems — have sensitivity rates from 94 to 100 percent. The higher the sensitivity, the less likely a test is to give a false negative result — saying someone doesn’t have antibodies when they really do. A person may also get a false negative result if they’re tested too early, before antibodies begin to accumulate around one to two weeks into an infection.
Part of the challenge with specificity in this context is that SARS-CoV-2 is not the only member of the coronavirus family to infect human beings. Two other coronaviruses, SARS and MERS, caused earlier multi-country outbreaks. Moreover, there are at least four coronaviruses that cause a fraction of cases of the common cold.
With SARS-CoV-2 so new, it’s hard to be sure. Not all infections create immunity; tetanus, for example, often doesn’t.
Those data seem to indicate that 4 to 5 percent of people in those places had already been exposed, giving Covid-19 a fatality rate closer to 0.1 to 0.2 percent. But those studies, which have not yet been reviewed by other scientists, have come under fire, partly due to the high rate of mistaken results in the test, which has not undergone FDA review and has a known tendency toward false positives.
This one is a really good read, packed with info
COVID-19 Antibody Testing: Tougher Than True/False
Antibodies should indicate if someone has had an infection in the past. But the promise of “immunity testing” is plagued by uncertainty about how the immune system responds to the coronavirus, as well as concerns about the tests’ accuracy.
www.discovermagazine.com
Why the Accuracy of SARS-CoV-2 Antibody Tests Varies So Much
The FDA cracks down on test makers as independent evaluations of their products' performance show a need for improvement.
www.the-scientist.com
New study confirms that 10 percent of the Stockholm population has antibodies against SARS-CoV-2
In the beginning of April, approximately 10 percent of Stockholm’s population had, at one point, formed antibodies against the virus causing COVID-19; according to a new study done by researchers […]
www.scilifelab.se
Coronavirus: surprisingly big problems caused by small errors in testing
A test that tells you with 94% accuracy that you have had coronavirus seems like a game-changer…until you do the maths.
No clue as we have nothing to compare it against. As I have said we will not honestly know until this time next year with the total death counts being mostly up to date through 2020. Hopefully the numbers can be reviewed and a new best practice going forward can be crafted so when the next pandemic hits we are not caught without toilet paper again.The status outlook is bought to us by a concerning study from our favorite unlockdownable friends the Swedes. Testing performed in April suggests by the end of that month only 7.3% of the residents of Stockholm had antibodies to defend them from COVID-19. They had been expecting closer to 20% by May 1st. If the results are correct and it is the case that such a small number acquire immunity with each wave, even rounding it up to an eventual 10% you are looking at perhaps five or six waves (years, if it's seasonal and strikes hardest in winter) before immune numbers are at the level where Heard Immunity (which they are definitely not trying to achieve) can defend the population, assuming the pathogen does not then mutate into another strain which will start the cycle all over again:
Just 7.3% of Stockholm had Covid-19 antibodies by end of April, study shows
Official findings add to concerns about Sweden’s laissez-faire strategy towards the pandemic
Does this set the front-loading-deaths theory back a bit...?
What I am finding interesting is the research is showing this virus was already out in the wild in a number of countries back in November well before it was even talked about being in China. It brings into question how effective it is shutting down air travel when it seems it happens far too late to do any good for the most part.
Past pandemics have also shown that infection rates are not a constant spread through the population. That they tend to form hot spots and do a lot of jumping around amongst a closed population. Some of it was attributed to the lack of traveling most of the populations did during the time periods but even within a city it was found that the spread was not even from an initial infection point but would flare up in sporadic pockets. This means unless you are testing a large enough sampling of a population the test results would be skewed one way or the other significantly.This is all still very much in the air. We're still playing on version 1.0 with antibody tests... there is still a lot of work to be done. Some good articles attached.
Understanding the startling rates of false positives and false negatives for tests that seem, on the surface, to be quite accurate could have profound consequences for health policy as we travel deeper into this pandemic. Failing to do our mathematical due diligence has the potential to take us past the tipping point beyond which the epidemic starts to grow again, leading to even more avoidable deaths.
The first commercial antibody tests to gain the FDA’s nod — from Cellex, Ortho Clinical Diagnostics and Chembio Diagnostic Systems — have sensitivity rates from 94 to 100 percent. The higher the sensitivity, the less likely a test is to give a false negative result — saying someone doesn’t have antibodies when they really do. A person may also get a false negative result if they’re tested too early, before antibodies begin to accumulate around one to two weeks into an infection.
Part of the challenge with specificity in this context is that SARS-CoV-2 is not the only member of the coronavirus family to infect human beings. Two other coronaviruses, SARS and MERS, caused earlier multi-country outbreaks. Moreover, there are at least four coronaviruses that cause a fraction of cases of the common cold.
With SARS-CoV-2 so new, it’s hard to be sure. Not all infections create immunity; tetanus, for example, often doesn’t.
Those data seem to indicate that 4 to 5 percent of people in those places had already been exposed, giving Covid-19 a fatality rate closer to 0.1 to 0.2 percent. But those studies, which have not yet been reviewed by other scientists, have come under fire, partly due to the high rate of mistaken results in the test, which has not undergone FDA review and has a known tendency toward false positives.
This one is a really good read, packed with info
COVID-19 Antibody Testing: Tougher Than True/False
Antibodies should indicate if someone has had an infection in the past. But the promise of “immunity testing” is plagued by uncertainty about how the immune system responds to the coronavirus, as well as concerns about the tests’ accuracy.
Why the Accuracy of SARS-CoV-2 Antibody Tests Varies So Much
The FDA cracks down on test makers as independent evaluations of their products' performance show a need for improvement.
New study confirms that 10 percent of the Stockholm population has antibodies against SARS-CoV-2
In the beginning of April, approximately 10 percent of Stockholm’s population had, at one point, formed antibodies against the virus causing COVID-19; according to a new study done by researchers […]
Coronavirus: surprisingly big problems caused by small errors in testing
A test that tells you with 94% accuracy that you have had coronavirus seems like a game-changer…until you do the maths.
Exactly, I agree... those pockets are going to vary from city to city, social group, employment group and so on.This means unless you are testing a large enough sampling of a population the test results would be skewed one way or the other significantly.
Also, I have heard the same thing regarding it being in the wild since November in China. I would swear up and down that I had it in February... whole family had it... it was a bad virus and took me almost 4 weeks to kick. Until I can get tested, nobody knows.
On that note:
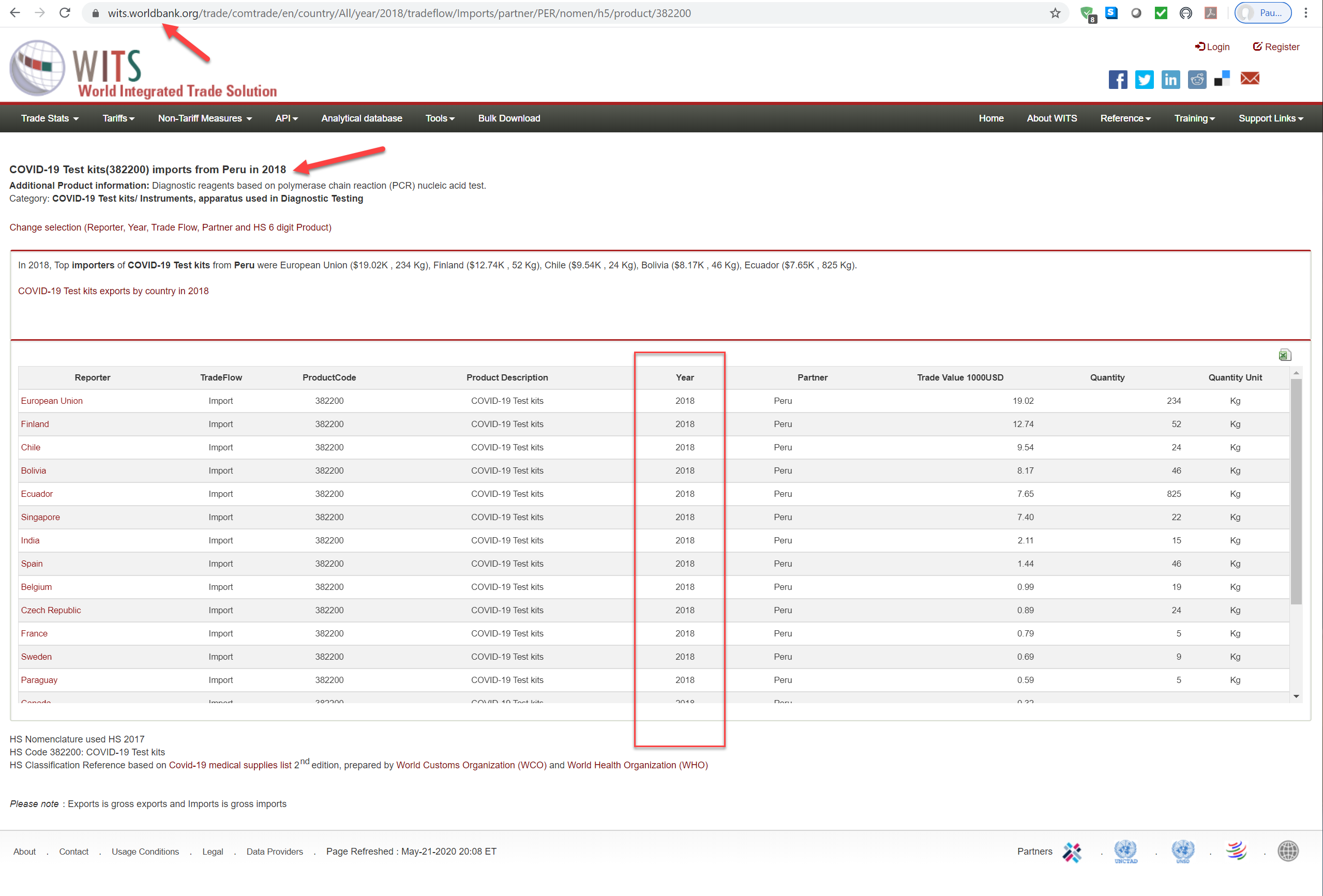
My wife told me on Sunday that she was worried because her sister in Peru says she has covid-19 symptoms. To make matters worse, she lives with my wife's parents in their late 70s. My wife said her sister could not get tested because they do not have tests available for her but she could get a private test for $1000 US, which is a lot of Peruvian money. Fortunately we have doctors in the family and she is being treated as if she has the virus. Still worried about my wife's parents - Not all Peruvians are so lucky. Let's just remember those less fortunate.
This looks odd. Worldbank WITS - is their data ok?

 datacatalog.worldbank.org
datacatalog.worldbank.org
World Integrated Trade Solution Trade Stats | Data Catalog
WITS Trade Stats is a database created by aggregating data from UN COMTRADE and UNCTAD TRAINS database. It provides information on bilateral trade exports, imports and tariffs for over 180 countries and regions.
AccidentProne8
Space Marshal
By the way, are you and Montoya debating something or just joking back and forth?This looks odd. Worldbank WITS - is their data ok?
World Integrated Trade Solution Trade Stats | Data Catalog
WITS Trade Stats is a database created by aggregating data from UN COMTRADE and UNCTAD TRAINS database. It provides information on bilateral trade exports, imports and tariffs for over 180 countries and regions.
View attachment 16090
I suppose you are talking about the arrogant statement (Sweden antilockdown)... I was joking/serious, I think Montoya was joking/serious... I think everyone else thought we were yelling at each other. This is actually a very talented and technical group talking about data, economics and so forth... everything related to the covid-19 experience play by play.By the way, are you and Montoya debating something or just joking back and forth?
Radegast74
Space Marshal
This was interesting, it shows what you can do when you have a functioning infectious disease plan/organized response, some discipline, and of course grunt work:
News summary of article:
 www.cnn.com
www.cnn.com
Article:

 wwwnc.cdc.gov
wwwnc.cdc.gov
News summary of article:
How a fitness class made 112 people sick | CNN
South Korea's aggressive testing and contact tracing program has given the country remarkable control of Covid-19, with the ability to respond quickly to new outbreaks, writes Kent Sepkowitz
www.cnn.com
Article:
Cluster of Coronavirus Disease Associated with Fitness Dance Classes, South Korea
COVID-19 Cluster Associated with Fitness Classes
Indeed I would say its because they have been dealing with SAR which is true but the sad part is SAR's and swine flue should have been a wake-up call to the rest of the world to make sure there was a plan in place for when it got out instead of this knee jerk reaction.This was interesting, it shows what you can do when you have a functioning infectious disease plan/organized response, some discipline, and of course grunt work:
News summary of article:
How a fitness class made 112 people sick | CNN
South Korea's aggressive testing and contact tracing program has given the country remarkable control of Covid-19, with the ability to respond quickly to new outbreaks, writes Kent Sepkowitz
Article:
Cluster of Coronavirus Disease Associated with Fitness Dance Classes, South Korea
COVID-19 Cluster Associated with Fitness Classes
I'm going to the gym within the week. I have lost all progress I made since I started in January but I have to get back at it. The gym I go to is a smaller gym and its either dead or has a bunch of old people in there for classes. Hopefully the old folks are staying away. If I'm going to get sick, I'm going to get sick from something I picked up from there because it's already happened twice, but ill let you know if I get the COVIDS.
As for me getting it and bringing it back to my family, for those of you that havent been following what I've been writing through this thread, I live with my 84 year old aunt and she has been going out and shopping anywhere they would let her ever since this began. Same with my 70 year old grandmother. As soon as this all started getting serious with the lockdowns, I swear they were compelled to go out even more. I have honestly been more worried about them coming home and giving it to me than I have of transmitting anything to them. If they were a kid during the war are they still considered a boomer or do they fall into the greatest generation.
Also, I'm still following this thread even though im not liking any posts or anything. I just don't have much to contribute atm, you all are covering the data points and other things fairly well.
I do have to say @ColdDog , I don't think youre the type to get offended so don't think I'm trying to be mean about this, but the way you write up / articulate your arguments seems to be like you don't take the time to fully flesh out what you want to say. Its apparent when you make posts back to back and why it seems like you have the most opposition of all the viewpoints in here. I share a lot of your views, but I keep my mouth shut for the most part because I'm not prepared to put the work in to articulate what I'm thinking and inject it into the middle of a discussion all the time. I know you are able to do so and I think people would be surprised if you took a bit more time to gauge who you're discussing things with and clarify your thoughts better.
I'm not saying I'm any better at any of this, but it's easy to point out your own shortcomings in others and I'd want someone to take the time to help me out if they thought I could use it. It's like the guy who lets you walk around with mustard on your beard beacause hes afraid of offending you. Like fuck off dude tell me the mustard is there and help a brother out!
Or you can tell me to fuck off which would also be understandable, who am I to say shit :P
As for me getting it and bringing it back to my family, for those of you that havent been following what I've been writing through this thread, I live with my 84 year old aunt and she has been going out and shopping anywhere they would let her ever since this began. Same with my 70 year old grandmother. As soon as this all started getting serious with the lockdowns, I swear they were compelled to go out even more. I have honestly been more worried about them coming home and giving it to me than I have of transmitting anything to them. If they were a kid during the war are they still considered a boomer or do they fall into the greatest generation.
Also, I'm still following this thread even though im not liking any posts or anything. I just don't have much to contribute atm, you all are covering the data points and other things fairly well.
I do have to say @ColdDog , I don't think youre the type to get offended so don't think I'm trying to be mean about this, but the way you write up / articulate your arguments seems to be like you don't take the time to fully flesh out what you want to say. Its apparent when you make posts back to back and why it seems like you have the most opposition of all the viewpoints in here. I share a lot of your views, but I keep my mouth shut for the most part because I'm not prepared to put the work in to articulate what I'm thinking and inject it into the middle of a discussion all the time. I know you are able to do so and I think people would be surprised if you took a bit more time to gauge who you're discussing things with and clarify your thoughts better.
I'm not saying I'm any better at any of this, but it's easy to point out your own shortcomings in others and I'd want someone to take the time to help me out if they thought I could use it. It's like the guy who lets you walk around with mustard on your beard beacause hes afraid of offending you. Like fuck off dude tell me the mustard is there and help a brother out!
Or you can tell me to fuck off which would also be understandable, who am I to say shit :P
Last edited:
UK numbers from today Friday 22nd May:
Total confirmed 254,195 with 3,287 new, total dead 36,393 with 351 new.
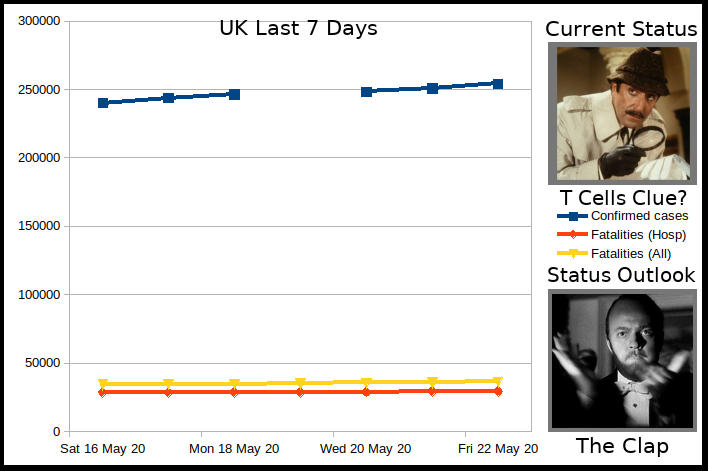
The current status is bought to us by research from over 60 of the worst effected cases showing a vital part of the immune system, T cells, were at a very low level between 200 and 800 per microlitre of blood, whereas you'd normally expect to see 2000 to 4000. Fascinating findings if correct and certainly raises a lot of questions if, for at least some, it does have an immune system suppression factor:
 www.bbc.co.uk
www.bbc.co.uk
The status outlook is bought to us by the originator of the clap for carers movement in the UK (where you go out on your doorstep at 8pm on a Thursday evening and clap for one minute as a mark of respect) who is calling for the tradition to end as it's going to be the 10th time next week and it is now for action to reward those working on the blunt end of the pandemic rather than just thanking them for it. They also stated in another interview it has become too politicized or used to carry unfocused messages "I think the narrative is starting to change and I don't want the clap to be negative."
 www.bbc.co.uk
www.bbc.co.uk
Total confirmed 254,195 with 3,287 new, total dead 36,393 with 351 new.
The current status is bought to us by research from over 60 of the worst effected cases showing a vital part of the immune system, T cells, were at a very low level between 200 and 800 per microlitre of blood, whereas you'd normally expect to see 2000 to 4000. Fascinating findings if correct and certainly raises a lot of questions if, for at least some, it does have an immune system suppression factor:
Coronavirus: Immune clue sparks treatment hope
Better understanding of Covid-19's impact on the immune system gives hope an existing drug might aid recovery.
The status outlook is bought to us by the originator of the clap for carers movement in the UK (where you go out on your doorstep at 8pm on a Thursday evening and clap for one minute as a mark of respect) who is calling for the tradition to end as it's going to be the 10th time next week and it is now for action to reward those working on the blunt end of the pandemic rather than just thanking them for it. They also stated in another interview it has become too politicized or used to carry unfocused messages "I think the narrative is starting to change and I don't want the clap to be negative."
Coronavirus: Clap for Carers should end, says founder
The nationwide applause has "had its moment" and should end after 10 weeks, Annemarie Plas says.
I have a lot of problems with the 'clap to thank' essential workers campaigns. I think it's a cheap way for governments and corporations to pass the 'responsibility of gratitude' to the public instead of doing the right thing. You know, providing proper PPE, work conditions, and hazard pay. It's great that guys like Captain Tom raised X amount for the NHS but the truth is, he shouldn't have to do that. Talk is cheap.The status outlook is bought to us by the originator of the clap for carers movement in the UK (where you go out on your doorstep at 8pm on a Thursday evening and clap for one minute as a mark of respect) who is calling for the tradition to end as it's going to be the 10th time next week and it is now for action to reward those working on the blunt end of the pandemic rather than just thanking them for it. They also stated in another interview it has become too politicized or used to carry unfocused messages "I think the narrative is starting to change and I don't want the clap to be negative."
Coronavirus: Clap for Carers should end, says founder
The nationwide applause has "had its moment" and should end after 10 weeks, Annemarie Plas says.
Radegast74
Space Marshal
Results of using remdesivir in a large scale, double-blind study:
Apparently, it works, but isn't that spectacular:
Apparently, it works, but isn't that spectacular:
Preliminary results from the 1059 patients (538 assigned to remdesivir and 521 to placebo) with data available after randomization indicated that those who received remdesivir had a median recovery time of 11 days (95% confidence interval [CI], 9 to 12), as compared with 15 days (95% CI, 13 to 19) in those who received placebo (rate ratio for recovery, 1.32; 95% CI, 1.12 to 1.55; P<0.001). The Kaplan-Meier estimates of mortality by 14 days were 7.1% with remdesivir and 11.9% with placebo (hazard ratio for death, 0.70; 95% CI, 0.47 to 1.04).
I know we havent been posting any opinion shows and the like, but this topic came up regarding people shaming those who want to open the economy. It aligns with what ive been worried about from the beginning and it addresses the things that I find concerning.
The easiest way to put it, is to ask "Why do they feel that way?"
The easiest way to put it, is to ask "Why do they feel that way?"
UK numbers from today Saturday 23rd of May:
Total cases 257,154 with 2,959 new, total dead 36,675 with 282 new.
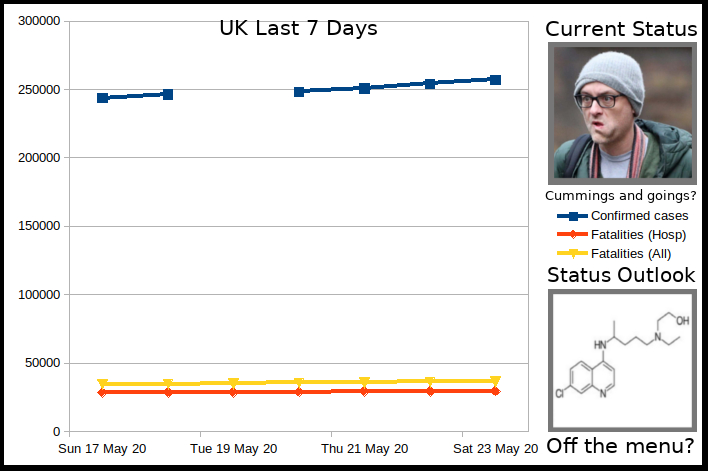
Todays status is bought to us by the UK Prime Ministers chief advisor Dominic Cummings (mastermind of the successful Brexit vote), who decided to take a 260 mile journey while under lockdown, with virus symptoms, his wife who also had symptoms, and their child to live with family in Durham, mere days after Boris Johnson fell victim to the pathogen:
 www.bbc.co.uk
www.bbc.co.uk
They have explained their actions as being essential as they were not going to be able to find child care if both he and his wife fell ill. One would assume however that as one of the top people in UK government and with an estimated 90% of the UK's population in the 260 mile radius from his London location, literally tens of millions of people (more if you include the countries accessible via Eurotunnel like France, the Netherlands and Belgium), it would not have been difficult for him to find child care a little closer to home given his means and position.
Persons in authority who have breached Lockdown such as Scotlands Chief Medical Officer (Went to their second home) and a scientist advising the government (His girlfriend popped round) both resigned immediately. Signs are there are no such plans for Mr. Cummings to follow suit or for those two persons and others besides to be reinstated now we know something as extraordinary as taking the virus 260 miles to another part of the country entirely can be justified.
The status outlook is bought to us by data collated from 96,000 COVID patents which suggests hydroxychloroquine does indeed increase the risk of death while suffering from COVID-19, in some cases with a fatality rate as high as one in four when combined with certain antibiotics. Apparently the rate without the drug is one in eleven.
 www.theguardian.com
www.theguardian.com
Although not a clinical trial, the findings suggest that this medicine would not stand out as something science would pick up on and investigate to see if it had beneficial effects. Until scientific trials have been concluded (including one to see if it could assist in stopping infection in the first place, which may be a possibility albeit one with as yet no stated evidence to base it on) this is the most compelling information that it may not be effective with this virus and may even hamper efforts to treat patients.
Total cases 257,154 with 2,959 new, total dead 36,675 with 282 new.
Todays status is bought to us by the UK Prime Ministers chief advisor Dominic Cummings (mastermind of the successful Brexit vote), who decided to take a 260 mile journey while under lockdown, with virus symptoms, his wife who also had symptoms, and their child to live with family in Durham, mere days after Boris Johnson fell victim to the pathogen:
Dominic Cummings: Did he break lockdown rules?
The UK PM's most senior adviser has responded to accusations that he broke lockdown rules - what did he say?
They have explained their actions as being essential as they were not going to be able to find child care if both he and his wife fell ill. One would assume however that as one of the top people in UK government and with an estimated 90% of the UK's population in the 260 mile radius from his London location, literally tens of millions of people (more if you include the countries accessible via Eurotunnel like France, the Netherlands and Belgium), it would not have been difficult for him to find child care a little closer to home given his means and position.
Persons in authority who have breached Lockdown such as Scotlands Chief Medical Officer (Went to their second home) and a scientist advising the government (His girlfriend popped round) both resigned immediately. Signs are there are no such plans for Mr. Cummings to follow suit or for those two persons and others besides to be reinstated now we know something as extraordinary as taking the virus 260 miles to another part of the country entirely can be justified.
The status outlook is bought to us by data collated from 96,000 COVID patents which suggests hydroxychloroquine does indeed increase the risk of death while suffering from COVID-19, in some cases with a fatality rate as high as one in four when combined with certain antibiotics. Apparently the rate without the drug is one in eleven.
Hydroxychloroquine: Trump's Covid-19 'cure' increases deaths, global study finds
Malaria drug should not be used to treat coronavirus, scientists say, after study shows high death rate
www.theguardian.com
Although not a clinical trial, the findings suggest that this medicine would not stand out as something science would pick up on and investigate to see if it had beneficial effects. Until scientific trials have been concluded (including one to see if it could assist in stopping infection in the first place, which may be a possibility albeit one with as yet no stated evidence to base it on) this is the most compelling information that it may not be effective with this virus and may even hamper efforts to treat patients.
Last edited: